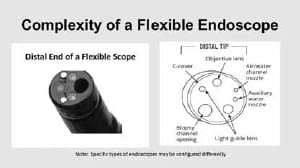
The Importance of Visual Inspection for Endoscope Reprocessing
Sri Mandava Infection Control Managing Endoscopes Patient Safety Regulatory Compliance Visual inspection has emerged in recent years as an important quality assurance step during endoscope reprocessing. Updated guidelines from AAMI, AORN and SGNA have all included a visual inspection step during the disinfection process to ensure that scopes are being thoroughly prepared for the next patient.
All three standards organizations have come out in support of adding the visual inspection in order to get a next level verification that all residual soil is removed during reprocessing. These visual inspections, in addition to cleaning verification tests, act as a check on an organization’s cleaning process. If scopes are continuously failing the cleaning verification or visual inspections, the reprocessing process may not be rigorous enough. This article by Mary Ann Drosnock at Healthcare Purchasing News summarizes what to look out for during a visual inspection:
“What are the kinds of evidence you should look for before endoscopes proceed to high-level disinfection? According to the guidelines, the endoscope should be inspected visually for conditions that could affect the disinfection process such as cracks, corrosion, discoloration, retained debris, and poor fiber optic illumination. Other items to inspect for, as noted by AORN, are cleanliness, missing parts, clarity of lenses, integrity of seals and gaskets, moisture, physical or chemical damage, and function. The use of magnification and adequate lighting does help assist in the visual inspection process to identify these abnormalities. These are the common warning signs that the scope is in need of repair or additional processing.
Other warning signs that an item may not be ready to be disinfected or sterilized are peeling of adhesives, cracks in lenses, brush gouge/scrape marks at the distal tip, stretched out covers on the bending section, and soil around or under the control knobs. Essentially, compare the scope to a new one and identify what is different. Then, evaluate if this could be a significant issue that may impact the ability of the scope to be cleaned, disinfected, or sterilized and could this be a risk to the patient?
There are other more obscure warning signs that the endoscope may need more attention or that reprocessing procedures are not in a state of control. Things like moisture retained in the channel upon inspection with a borescope after disinfection would tell you that your drying processes are not adequate. Retained lint/fibers are also very commonly seen upon inspection with a borescope and would bring to light the possible practice that staff members are not using lint-free or low-linting clothes or sponges during reprocessing. Retained brush bristles would warrant investigating the condition of reusable brushes or the possible practice of reusing single-use brushes mistakenly. Internal channels that are heavily damaged by gouging or scraping may warrant taking a look at the physician practices with endoscope accessories, such as keeping the distal tip angulated while passing or removing a biopsy forceps.
Use of a borescope for inspection of internal channels of the endoscopes is an additional step that may be taken to engineer quality into an endoscope’s reprocessing program. Both ST911 and AORN endoscope guidelines do highlight the process within their document. For example, AORN states that “Internal channels of flexible endoscopes may be inspected using an endoscopic camera or borescope. [2: High Evidence] Endoscopic cameras and borescopes penetrate the lumen and allow for improved visual inspection. Certainly, inspection of the internal channels with a borescope is a quality-driven process and will help a facility to assess the condition of their endoscopes, the overall reprocessing procedures and potentially the drying process. The one issue that is often raised with inspection with borescopes is when to perform this process.
Many facilities inspect their scopes periodically after the disinfection process is complete and the scopes are in storage. If doing this, then the scope should be reprocessed again before use. By performing inspection at this stage in the process, a facility can assess their internal drying practices and clearly determine whether it is currently being performed adequately or not. According to SGNA, scopes must be completely dry prior to storage or should not be used on patients without being reprocessed again. Other facilities will inspect with a borescope after manual cleaning prior to disinfection or sterilization. Although this is an option, the scopes are highly contaminated at this point and completely wet internally. A complete drying procedure would need to be initiated after cleaning in order to inspect with the borescope. If not, all that will be seen is water, which is not helpful.
Therefore, to perform a visual inspection, at a minimum the unaided eye should be used to inspect the external surfaces of the endoscope after manual cleaning. Additionally, current standards and guidelines do call for the additional use of lighted magnification to be added to the process of visual inspection. The process of performing cleaning verification is also clearly warranted based upon the current standards and guidelines. Borescopic examination of internal channels is a newer process, but one that is recommended within AAMI ST911 and AORN endoscope guidelines.”
https://www.mobileaspects.com/the-importance-of-visualinspection- for-endoscope-reprocessing/
October 30, 2017